Sleeve Gastrectomy
Laparoscopic sleeve gastrectomy surgery
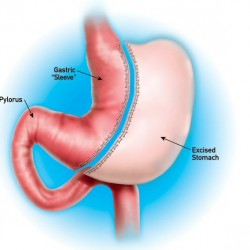
The vertical sleeve gastrectomy (also called sleeve gastrectomy, vertical gastrectomy or gastric sleeve) is a procedure that induces weight loss by decreasing the amount of food you can eat at a time. In the sleeve gastrectomy surgery, approximately 80% of the total stomach is removed, therefore reducing the capacity of the stomach to store food. In other words, it is another restrictive bariatric operation.
In the sleeve gastrectomy procedure, approximately 80% of the total stomach is removed, therefore reducing the capacity of the stomach to store food.
The sleeve gastrectomy operation was originally intended for super-obese or high-risk patients with the intention of performing an additional weight loss procedure at a later time. However, patients lost weight and were happy with their results and did not need a second operation.
The sleeve gastrectomy is currently recommended if you eat large portions of food or if you need to lose a large amount of weight. The operation can be completed through laparoscopic or open surgery.
The sleeve gastrectomy works similarly to the gastric banding. You eat small amounts of food, you feel full, you stop eating, and you lose weight without feeling hungry. While the stomach is reduced in size, the stomach outlet and the nerves to the stomach remain intact; therefore its function is preserved. You will have a normal digestion of nutrients and you will not need nutritional supplements afterwards. Similar to the gastric bypass, the sleeve gastrectomy operation is not reversible.
While the stomach is reduced in size, the stomach outlet and the nerves to the stomach remain intact; therefore its function is preserved. You will have a normal digestion of nutrients and you will not need nutritional supplements afterwards.
The vertical sleeve gastrectomy operative technique
The vertical sleeve gastrectomy can be performed using laparoscopic surgery. All patients are given blood thinners and IV antibiotics before surgery. Additionally, you will have compressive stockings and an intermittent compressive device in your legs until you are completely recovered.
The technique for the sleeve gastrectomy involves 5 small incisions through which a camera and small instruments are introduced into the abdomen. The surgery takes about one hour and a half and it requires general anesthesia.
A tube is passed from the esophagus into the duodenum (the first portion of the small bowel) and it is used to calibrate the diameter of the stomach that will be left in place. The stomach is then divided using staplers in an upward direction removing the portion of the stomach that enlarges when you eat food. Therefore, a thin portion of the stomach in the form of a cylinder or a “sleeve” is left in place. We use sutures to reinforce the staples to reduce the risk of bleeding or a leak. The small bowel is not divided.
Unlike the gastric bypass, in the sleeve gastrectomy there are no connections between the stomach and the intestine. Therefore, there is a much smaller risk of having a postoperative leak. Also, because of the shorter anesthesia time compared to the gastric bypass, patients undergoing sleeve gastrectomy have fewer postoperative pulmonary complications.
Unlike the gastric bypass, in the sleeve gastrectomy there are no connections between the stomach and the intestine. Therefore, there is a much smaller risk of having a postoperative leak.
This operation can also be done through open conventional surgery in order to decrease costs. Open surgery might also be indicated in patients with multiple abdominal operations. Also, it can be done in patients with a successful gastric banding but have developed complications or have regained weight.
Recovery from sleeve gastrectomy surgery
Regardless of the technique used to complete the sleeve gastrectomy, you will be able to get out of bed the night of the operation. However, you will be kept without eating or drinking water for 48 hours. All medications and liquids will be given through the IV. After this period, you will be able to drink water. You will be kept in the hospital for an additional 24 hours to make sure there are no problems drinking liquids and you will be discharged to your hotel with the diet recommended by the dietitian. You will be back to your routine daily activities on an average of 6 to 8 days following surgery.
Diet after sleeve gastrectomy surgery
After the sleeve gastrectomy surgery you will have a strict follow-up with the dietitian. Once you restart your diet 48 hours after your operation, you will only be able to drink water. The next day you will be started on a full liquid diet including protein supplements to enhance your wound healing. You will have this diet for at least two weeks. You will then be advanced to pureed-type diet for the following three. Depending on your progress, solid food will be reintroduced about five weeks following surgery. Nutritional supplements are not required following sleeve gastrectomy.
Our experience
Dr. Rodrigo Gonzalez is one of the very few surgeons practicing in Latin America who completed a supervised one-year fellowship program at a University-affiliated hospital in the United States. He is also one of the few surgeons in Latin America performing sleeve gastrectomy operations. His training involved the evaluation and preparation of clinically significant obese patients for weight-loss surgery. During his training, Dr. Rodrigo Gonzalez acquired sufficient experience and knowledge to be able to manage and treat patients with morbid obesity and to perform these operations here in the United States and any other country in the world.
Dr. Rodrigo Gonzalez is one of very few surgeons in Latin America who performs sleeve gastrectomy operations.
Since his return to Guatemala, Dr. Rodrigo Gonzalez has dedicated most of his practice to bariatric surgery and has done well over hundreds of bariatric operations including Roux-en-Y gastric bypass, gastric banding, sleeve vertical gastrectomy, and revision of complicated or failed weight-loss operations to Roux-en-Y gastric bypass.
Dr. Rodrigo Gonzalez dedicated a significant amount of his time to study and research the field of Bariatrics. He has published over 25 papers in the most prestigious medical international journals and has been asked to write chapters for 5 books published in the United States and Great Britain. He has also been invited to publish review articles in renowned medical journals. He is considered by the international medical community as an expert in bariatric surgery and is therefore frequently asked to give talks in bariatric courses and meetings in order to present his experience in weight-loss surgery.